Original Research Article
Year: 2016 | Month: July-September | Volume: 1 | Issue: 3 | Pages: 53-63
Prevalence and Determinants of Adolescent Malnutrition in Owerri, Imo State, Nigeria
Chukwuma B. Duru1, Anthony C. Iwu2, Kenechi A. Uwakwe1, Kevin C. Diwe1, Chinomnso C. Nnebue3, Irene A. Merenu1, Kinsley Achigbu4, Henry N. Chineke1
1Department of Community Medicine, Imo State University, Owerri, Imo State, Nigeria.
2Department of Community Medicine, Imo State University Teaching Hospital, Orlu Imo State, Nigeria.
3Dept of HIV Care and Community Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria.
4Department of Paediatrics and Child Health, Federal Medical Centre Owerri, Imo State, Nigeria.
Corresponding Author: Chukwuma B. Duru
ABSTRACT
Background: Adolescence is a transitional period of rapid growth and increased nutrient demand and also, a window of opportunity to correct existing nutritional problems inherited from childhood; but unfortunately, it appears that, the least attention in terms of nutritional interventions is given to the adolescents.
Objective: To determine the prevalence and determinants of adolescent malnutrition in Owerri, Imo State. Nigeria.
Materials and Methods: A cross sectional descriptive design using a multistage sampling technique, was used to select 504 adolescents aged 10-19 years old from both public and private secondary schools in Owerri municipal Local Government Area. Data was collected using a pretested semi structured interviewer administered questionnaire. Descriptive analysis was carried out using computer software (SPSS version 20). Chi square statistics were computed to determine significant relationships while multiple logistic regressions were used to determine the predictors of adolescent malnutrition. P value was set at 0.05 significant level.
Results: The results revealed that 18.6% and 11.6% of adolescents were underweight and overweight/obese respectively and that a majority of the respondents (89.6%) had a poor to fair level of knowledge about overweight and obesity. There were statistically significant relationships between adolescent nutritional status and age of adolescents (p=0.000), gender (p=0.004), religion (p=0.010), caregiver (p=0.000), occupation of the caregiver (p=0.000), class level in school (p=0.000) and birth position of the adolescent in the household (p=0.000). It was further revealed that adolescents aged 14-16 and 17-19 years old, who were first born, female, with orthodox religious background and are senior students in school were significantly more likely to be overweight/obese than underweight. (p<0.05)
Conclusion: There should be an increased focus on adolescent nutrition and as a consequence, accessible, appropriate and effective integrated nutritional strategies should be developed to tackle the increasing malnutrition problems facing the adolescent.
Keywords: Prevalence, determinants, malnutrition, adolescents, Owerri, Nigeria.
1.0 INTRODUCTION
Malnutrition is a state of poor nutrition due to dietary intakes that are either above or below the optimal dietary level. [1]
It remains an ongoing, significant, global public health problem with its prevalence and patterns differing between countries and regions; and it is now becoming increasingly apparent in adolescents, especially in developing countries where they are more vulnerable to nutritional deficiencies as a result of early childhood nutritional problems of underweight, stunting and wasting. [2]
Adolescence is a period of transition between childhood and adulthood and also a time of rapid growth accompanied by an increase in nutrient demand which may be affected by unfavourable environmental conditions, socioeconomic status, lifestyle, eating habits and the level of physical activity. It comprises individuals between the ages of 10 and 19 years old that make up approximately 20% of the world’s population with about 90% of them living in low and middle-income countries and who appear to remain a neglected, difficult to measure and hard to reach population.[3-5]
Underweight and overweight reflects malnutrition and many boys and girls in developing countries enter adolescence, undernourished, as a previous WHO report [5]
observed that, under-nutrition was widespread among Nigerian adolescents, with wasting and stunting being more frequent in the rural areas. But now, in addition, an increasing number of adolescents are becoming overweight or obese especially in low income countries.[6]
The coexistence of overweight/obesity and underweight appears to be common in developing countries as a recent study in Nigeria, further highlights the double burden of over and under nutrition both occurring among the adolescents. [7,
8]
Abah et al, [9]
reported the prevalence of underweight, overweight and obesity among secondary school students in a peri-urban Nigerian town to be 6.0%, 8.6% and 1.0% respectively with gender, type of school and social class of the family influencing the patterns of malnutrition.
The challenges of poor nutrition continues throughout the cycle of life, with the adolescent period being a critical pivotal stage, for the provision of adequate and appropriate dietary nutrition due to the accelerated physical growth, development and its associated increased nutritional needs. Despite this, it appears that the least attention is given to the adolescent stage in terms of nutritional interventions when compared to preschool children and pregnant women. As a consequence, especially for adolescent girls who become mothers, the vicious cycle of intergenerational malnutrition is perpetuated. [10]
Adolescence is a window of opportunity to correct existing nutritional problems from childhood, and to influence healthy eating and lifestyle behaviors, in order to prevent the emergence of future chronic diseases. This will reduce the substantial risk of morbidity and mortality, with the intention of preparing the adolescent nutritionally, as a foundation for good health in adult life. [6]
As part of the integrated management of adolescent nutrition, appropriate nutritional assessments are required which are associated with specific challenges due to the fact that, anthropometric assessments in adolescents are more complex than in children, because of the rapid growth patterns and variations that occur during the adolescent period and more specifically, due to the unavailability of appropriate local adolescent anthropometric data, as reference population. Nevertheless, a World Health Organization (WHO) Expert Committee recommended BMI for age as the best indicator of thinness in adolescence for which, the reconstructed 1977 National Center for Health Statistics (NCHS)/WHO growth charts (2007 WHO reference growth charts) is to be used as a reference to assess the nutritional status of adolescents. [11-13]
In addressing the nutrition health problems of adolescents, it is critically important to understand the prevalence and the determinants of adolescent malnutrition in order to develop specific, effective strategies with an integrated approach of promotion, prevention and treatment with multiple care entry points that will further overcome some of the barriers to health access, that appears to be usually encountered by adolescents; which is what our research sets to achieve.
2.0 METHODOLOGY
2.1 Study Area
The study was conducted in Owerri municipal Local Government Area (LGA), one of the three LGA’s that make up Owerri city in Imo State, South East Nigeria. It had a total population of 125,337 (60,882 males and 64,455 females) by 2006 census, with a State annual growth rate of 3.2%.The LGA occupies an area of 58.5 square kilometres with a population density of about 2,143 persons per square kilometre. [14]
It is an urban setting and also the capital of the State.
2.2 Study Population/Study design/Selection criteria
The study population comprised male and female adolescents (10-19 years old) in public and private secondary schools in Owerri municipal LGA of Imo State. The study design was a Cross Sectional Descriptive Study. Inclusion criteria was; any adolescent aged between 10 and 19 years attending school in the selected secondary schools and the exclusion criteria was; any selected adolescent that had any form of physical challenge or was a visitor at the time of the study.
2.3 Sample Size Estimation
The minimum sample size was calculated using the Cochrane formula. [15]
![]()
When n= minimum sample size, Z= Standard normal deviate corresponding to 5 % significant level, p = proportion of adolescent population with malnutrition in a Nigerian study [16]
was 14.2%, q=1-p, d= tolerable error of margin set at 0.05, Z=1.96, q=1-0.142. Applying the formula above, the calculated minimum sample size was 187 but a sample size of 501 participants was used in this study.
2.4 Sampling Technique
The sampling technique used to select the adolescents from public and private secondary schools in Owerri municipal LGA was a multistage sampling technique. The first step involved the stratification of the secondary schools into public and private schools. There were 9 schools in each stratum. The next step involved the selection of 2 schools each from the public and private secondary schools using simple random sampling by balloting. The last step involved selection of all the students between the ages of 10 and 19 years old in attendance at the time of study visit from each of the four schools. Those who refused to participate were not included.
2.5 Data Collection and Analysis
Data was collected using a pretested, semi structured, interviewer administered questionnaire. The questionnaire comprised2 sections; section one: the socio-demographic characteristics including weight and height measurements and section two: the awareness and knowledge of obesity. Research assistants were used to collect information from the participants. Data was collected from the participants by face to face interview.
The level of awareness and knowledge of obesity was determined by scoring the questions that assessed awareness and knowledge. For a single response question, a correct answer was scored 1; a false answer was scored 0. For a multiple response question, each correct answer was scored 1 and up to a maximum of 3 correct answers, a subtotal score of 3 was allocated and for a false answer, 0 was allocated. The total maximum score for all the correct answers for assessing the level awareness and knowledge was 40. The aggregate score for each respondent according to the level of awareness and knowledge was translated to a percentage and assessed against a scale of 0-49% for poor, 50-69% for fair and 70% or more for good.
The weight in kilograms (Kg) was taken using a digital weighing scale and the height in metres (m) using a floor type height scale. The nutritional status was determined using Body Mass Index (BMI) = kg/m2. The BMI, calculated for a participant of a given gender and age, was interpreted relative to the 2007 WHO reference z- score growth chart for that gender. The participants were then classified into one of the following categories; Underweight: less than -2 Standard deviations, Normal weight: between -2 and +1 Standard deviations and Overweight/Obese: above +1 Standard deviations.
Data was cleaned and validated manually, and analysed using SPSS v22. Descriptive statistics (frequency tables and summary indices) were generated. Chi Square was used to test association between categorical variables, while multiple logistic regression was used to determine the predictors of adolescent malnutrition. P value was set at 0.05 significant level.
2.6 Ethical Considerations
Ethical approval was obtained from the Ethics Committee of the Department of Community Medicine, Madonna University Elele, Rivers State. All authors hereby declare that the study has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Five hundred and one students were selected. All the questionnaires were completely and correctly filled with a response rate of 100%.
3.1 Sociodemographic Characteristics of respondents
The mean age of the respondents was 14.96±2.08 years old with male to female ratio of 1:1.5 and close to half belonging to the Catholic faith (46.1%).
Most of the respondents were from monogamous families (82%) with their parents (79%) as principal caregivers who were either traders or civil servants (62%)
More than half of the respondents were either the 2nd, 3rd or 4th child (58.7%) or having more than 4 siblings in the family (55.7%). Also more than half of the respondents (53.5%) attended private secondary schools with majority of them (74.9%) being in senior classes (Table 1).
Table 1: Sociodemographic Characteristics
Variable |
Category |
Frequency (%) |
Age (years) |
10-13 |
103(20.5) |
14-16 |
299(59.7) |
|
17-19 |
99(19.8) |
|
Gender |
Male |
203(40.5) |
Female |
298(59.5) |
|
Religion |
Catholic |
231(46.1) |
Pentecostal |
189(37.7) |
|
Orthodox |
75(15.0) |
|
Others |
6(1.2) |
|
Caregiver |
Parents |
396(79.0) |
Guardian |
83(16.6) |
|
Relatives |
24(4.4) |
|
Occupation caregiver |
Trading |
164(32.7) |
Civil servant |
147(29.3) |
|
Professional/teacher |
118(23.6) |
|
Farmer/artisan |
46(9.2) |
|
Others |
26(5.2) |
|
Type of school |
Private |
268(53.5) |
Public |
233(46.5) |
|
Class level |
Junior |
126(25.1) |
Senior |
375(74.9) |
|
Type of family |
Monogamous |
411(82.0) |
Polygamous |
90(18.0) |
|
Number of siblings |
1-4 |
222(44.3) |
>4 |
279(55.7) |
|
Position in Household |
1st |
128(25.5) |
2nd-4th |
294(58.7) |
|
>4th |
42(8.4) |
|
Last |
37(7.4) |
Table 2: Awareness and Knowledge of Overweight/Obesity
Variable |
Category |
Frequency (%) |
Awareness of |
Yes |
470(93.8) |
No |
31(6.2) |
|
*Understanding of |
A fat person |
344(73.2) |
Eating too much |
207(44.0) |
|
Enjoyment/good living |
48(10.2) |
|
Big and Tall |
28(6.0) |
|
Others |
4(0.9) |
|
*Sources of |
Teachers |
260(55.3) |
Television |
210(44.7) |
|
Parents/relatives |
207(44.0) |
|
Newspaper |
183(38.9) |
|
Radio |
148(31.5) |
|
Books |
117(24.9) |
|
Friends/Schoolmates |
98(20.9) |
|
Health personnel |
93(19.8) |
|
Others |
10(2.1) |
|
*Causes of |
Lack of exercise |
323(68.7) |
Excessive eating |
249(53.0) |
|
Familial |
111(23.6) |
|
Eating fast foods |
49(10.4) |
|
Drugs |
24(5.1) |
|
Others |
14(3.0) |
|
*Problems of
|
Low self-esteem |
190(40.4) |
Sleep apnoea |
177(37.7) |
|
Hypertension |
159(33.8) |
|
Diabetes mellitus |
159(33.8) |
|
Osteoarthritis |
157(33.4) |
|
Body odour |
152(32.3) |
|
Heart problems |
104(22.1) |
|
Sudden death |
56(11.9) |
|
Skin infection |
42(8.9) |
|
Others |
40(8.5) |
*Multiple responses
3.2 Awareness and Knowledge of Overweight/Obesity
Most of the respondents (93.8%) were aware of overweight/obesity and a majority of those aware, (73.2%) referred to it as “any person that is fat” with more than half of the respondents (55.3%) reporting that their main source of information about overweight and obesity came from their teachers in school. While close to three quarters of the respondents (68.7%) attributed overweight and obesity to lack of exercise, just over half of the respondents (53%) attributed it to excessive eating. Furthermore, while over one third of the respondents, reported low esteem (40.4%) and sleep apnoea (37.7%) as problems of overweight and obesity, just about one third reported hypertension (33.8%) and diabetes (33.8%) as problems of overweight and obesity (Table 2).
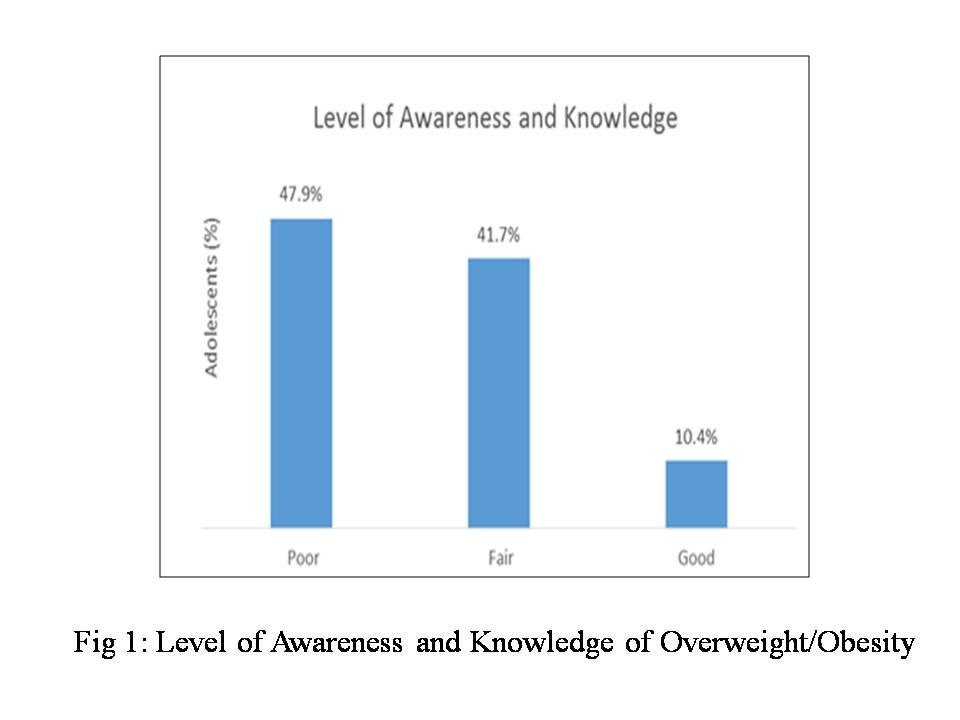
Fig 1: Level of Awareness and Knowledge of Overweight/Obesity
{kind=link}
Consequently, the majority of the respondents (89.6%) had a poor to fair level of awareness and knowledge of overweight and obesity (Fig 1).
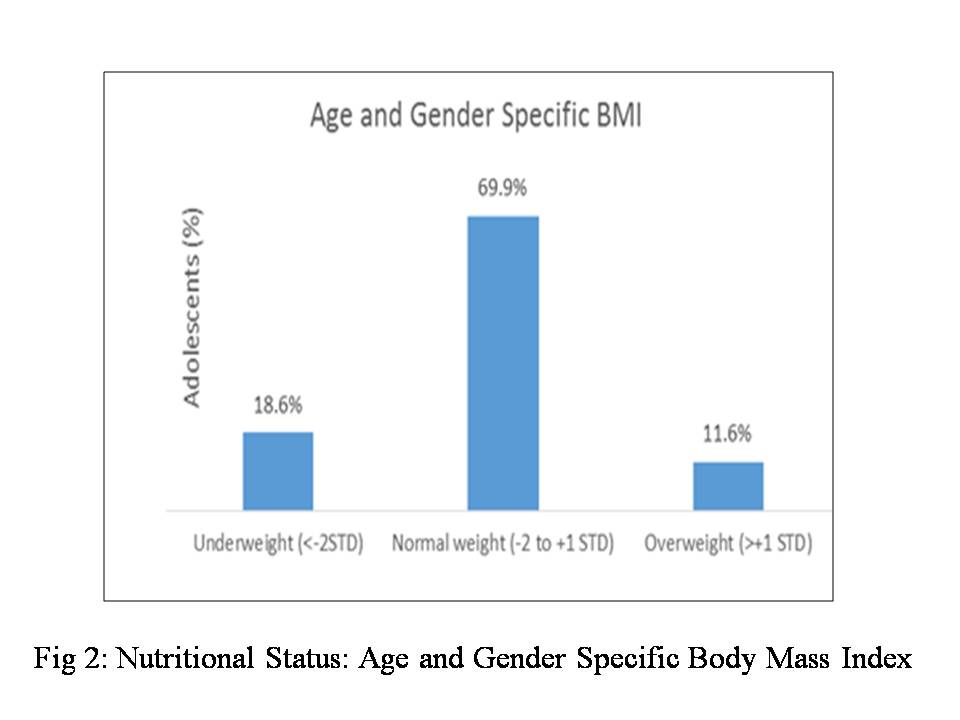
3.3 Nutritional Status; Weight, Height and Body Mass Index of respondents
Most of the respondents weighed between 41-80kg (87.4%) and had a height measurement of 141-180cm (96.4%) (Table 3)
According to the BMI for age and gender, a majority of the respondents (70%) were considered as having normal weight i.e. between -2 to +1 Standard deviation of the 2007 WHO reference growth charts and about 30% of respondents were malnourished (underweight and overweight/ obese) (Fig 2).
Table 3: Weight and Height measurements of respondents
Variable |
Category |
Frequency (%) |
Weight (Kg) |
21-40 |
48(9.6) |
41-60 |
311(62.1) |
|
61-80 |
127(25.3) |
|
>80 |
15(3.0) |
|
Height (cm) |
121-140 |
10(2.0) |
141-160 |
230(45.9) |
|
161-180 |
253(50.5) |
|
>180 |
8(1.6) |
Fig 2: Nutritional Status: Age and Gender Specific Body Mass Indexo
{kind=link}
3.4 Factors Associated with Nutritional Status of respondents
The following factors were significantly associated with the nutritional status of adolescents; Age (p=0.000), Gender (p=0.004), Religion (0.010), Caregiver (0.000), Occupation of caregiver (0.000), Class level (0.000) and Position in household (0.000). While on the other hand; Type of school, Type of family and Number of siblings were not significantly associated (p>0.05) (Table 4).
Table 4: Factors associated with Nutritional Status of respondents
Variable |
Underweight (%) |
Normal (%) |
Overweight/Obesity (%) |
Total (%) |
χ2 |
df |
p-value |
Age (yrs) |
52.68 |
4 |
0.000* |
||||
10-13 |
44(42.7) |
54(52.4) |
5(4.9) |
103(100) |
|||
14-16 |
36(12.0) |
226(75.6) |
37(12.4) |
299(100) |
|||
17-19 |
13(13.1) |
70(70.7) |
16(16.2) |
99(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Gender |
11.18 |
2 |
0.004*
|
||||
Male |
43(21.2) |
148(72.9) |
12(5.9) |
203(100) |
|||
Female |
50(16.8) |
202(67.8) |
46(15.4) |
298(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Religion |
16.80a |
6 |
0.010* |
||||
Catholic |
43(18.6) |
164(71.0) |
24(10.4) |
231(100) |
|||
Pentecostal |
37(19.6) |
135(71.4) |
17(9.0) |
189(100) |
|||
Orthodox |
9(12.0) |
50(66.7) |
16(21.3) |
75(100) |
|||
Others |
4(66.7) |
1(16.7) |
1(16.7) |
6(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Caregiver |
44.92 |
4 |
0.000*
|
||||
Parents |
70(17.7) |
281(71.0) |
45(11.4) |
396(100) |
|||
Guardians |
8(9.6) |
66(79.5) |
9(10.8) |
83(100) |
|||
Relatives |
15(68.2) |
3(13.6) |
4(18.2) |
22(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Occupation caregiver |
46.98 |
8 |
0.000* |
||||
Traders |
26(15.9) |
121(73.8) |
17(10.4) |
164(100) |
|||
Civil servants |
27(18.4) |
104(70.7) |
16(10.9) |
147(100) |
|||
Professional/ teacher |
14(11.9) |
83(70.3) |
21(17.8) |
118(100) |
|||
Farmer/artisan |
9(19.6) |
34(73.9) |
3(6.5) |
46(100) |
|||
Others |
17(65.4) |
8(30.8) |
1(3.8) |
26(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
School type |
2.08 |
2 |
0.354
|
||||
Private |
45(16.8) |
188(70.1) |
35(13.1) |
268(100) |
|||
Public |
48(20.6) |
162(69.5) |
23(9.9) |
233(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Class level |
78.37 |
2 |
0.000*
|
||||
Senior |
37(9.9) |
284(75.7) |
54(14.4) |
375(100) |
|||
Junior |
56(44.4) |
66(52.4) |
4(3.2) |
126(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Family type |
5.70 |
2 |
0.058
|
||||
Monogamous |
69(16.8) |
296(72.0) |
46(11.2) |
411(100) |
|||
Polygamous |
24(26.7) |
54(60.0) |
12(13.3) |
90(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Number of siblings |
0.08 |
2 |
0.961 |
||||
1-4 |
40(18.0) |
156(70.3) |
26(11.7) |
222(100) |
|||
>4 |
53(19.0) |
194(69.5) |
32(11.5) |
279(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
Birth position in Household |
68.06 |
6 |
0.000* |
||||
1st |
19(14.8) |
92(71.9) |
17(13.3) |
128(100) |
|||
2nd-4th |
39(13.3) |
230(78.2) |
25(8.5) |
294(100) |
|||
>4th |
19(45.2) |
19(45.2) |
4(9.5) |
42(100) |
|||
Last |
16(43.2) |
9(24.3) |
12(32.4) |
37(100) |
|||
Total |
93(18.6) |
350(69.9) |
58(11.6) |
501(100) |
|||
* Statistically Significant, a- Likelihood ratio
3.5 Predictors of Adolescent Malnutrition using Multiple Regressions
Adolescents aged 14-16 and 17-19 years old were significantly more likely to be overweight/obese than underweight when compared to adolescents aged 10-13 years old. (OR: 9.044; 3.2207-25.3989, p=0.000) and (OR: 10.831; 3.3297-35.2300, p=0.000) respectively. Female adolescents were significantly more likely to be overweight/obese than underweight when compared to the male adolescents. (OR: 3.297; 1.5497-7.0131, p=0.001). Adolescents whose religion is orthodox, were significantly more likely to be overweight/obese than underweight when compared to adolescent Catholics. (OR: 3.185; 1.2229-8.296, p=0.015). The adolescent, whose caregiver’s occupation is neither a civil servant, professional, teacher, farmer nor artisan was significantly less likely to be overweight/obese than underweight when compared to adolescents whose caregivers occupation is trading. (OR: 0.09; 0.0109-0.7402, p=0.008). Similarly, adolescents who are in junior classes and in the 5th or more birth position among the siblings in the household are significantly less likely to be overweight/obese than underweight when compared to adolescents in senior classes (OR: 0.049; 0.0163-0.1466, p=0.000) and in the 1stbirth position among the siblings in the household (OR: 0.235; 0.0667-0.8305, p=0.020) respectively (Table 5).
Table 5: Predictors of Malnutrition (underweight and overweight/obese)
Variable |
OR(estimate) |
95 (CI) |
p-value |
Age (years) |
|||
10-13 |
1.000 |
- |
|
14-16 |
9.044 |
3.220725.3989 |
0.000* |
17-19 |
10.831 |
3.329735.2300 |
0.000* |
Gender |
|||
Male |
1.000 |
- |
|
Female |
3.297 |
1.5497-7.0131 |
0.001* |
Religion |
|||
Catholic |
1.000 |
- |
|
Orthodox |
3.185 |
1.2229-8.296 |
0.015* |
Pentecostal |
0.823 |
0.3846-1.7621 |
0.617 |
Others |
0.448 |
0.0473-4.2392 |
0.652 |
Caregiver |
|||
Parents |
1.000 |
- |
- |
Guardians |
1.750 |
0.6289-4.8695 |
0.279 |
Relatives |
0.415 |
0.1294-1.3296 |
0.129 |
Occupation of caregiver |
|||
Traders |
1.000 |
- |
- |
Civil servants |
0.906 |
0.3799-2.1623 |
0.823 |
Professional/ teacher |
2.294 |
0.9219-5.7086 |
0.072 |
Farmer/artisan |
0.510 |
0.1205-2.1573 |
0.502 |
Others |
0.09 |
0.0109-0.7402 |
0.008* |
Class level |
|||
Senior |
1.000 |
- |
- |
Junior |
0.049 |
0.0163-0.1466 |
0.000* |
Birth position in Household |
|||
1st |
1.000 |
- |
- |
2nd-4th |
0.716 |
0.3140-1.6345 |
0.427 |
>4th |
0.235 |
0.0667-0.8305 |
0.020* |
Last |
0.838 |
0.3102-2.2653 |
0.729 |
* Statistically Significant.
4.0 DISCUSSION
This study determined the prevalence and assessed the determinants of malnutrition in adolescents and it revealed that 18.6% and 11.6% of adolescents were underweight and overweight/obese respectively. It also revealed that age, gender, religion, which the caregiver is occupation of the caregiver, class level in school and birth position of the adolescent in the household was significantly associated with the nutritional status of the adolescent. It was further determined that an adolescent above the age of 13 years old, female, the first child in the family, a senior student in school, with an orthodox religious background and whose caregiver is a trader is significantly more likely to be overweight/obese than underweight.
The prevalence of underweight among adolescents observed in the present study, was similar to the observations of studies done in Mozambique, Kenya and in Osun and On do States of Nigeria [17-20]
that reported prevalence rates of between 16-20% but this was contrary to what was observed in studies done in Cameroon, Benin and Senegal [21-23]
that reported prevalence rates of 4%, 23% and 29.8% respectively and also in studies done in Edo, Lagos and Abia States of Nigeria,[9,
24,
25]
that reported even lower prevalence of 2.6%, 3% and 6% respectively. Though a previous study by Brabin et al, [26]
showed that Nigerian adolescents experience widespread under nutrition with the prevalence ranging from 8% in the urban areas to 16% in the rural areas, which was further supported by a study done in four urban towns in southern Nigeria [16]
with a prevalence of 8.3%, these observations were not consistent with the present study which was also conducted in an urban area that showed a prevalence of 18.6% under nutrition among the adolescents. This probably could be explained by the present deteriorating economic conditions being currently observed in the country with the impact appearing to be worse in the urban areas.
The observed difference between the prevalence of underweight and overweight/obesity with the predominance of underweight in the present study, has been previously observed by Prentice in 2006, [27]
who reported, that even though overweight and obesity is a major concern in developed countries, nevertheless, in the developing countries, it is still an increasing concern with under nutrition being more prevalent.
The present study, further highlights this increasing concern of overweight and obesity in developing countries and with a prevalence of 11% among adolescents, it appears to be consistent with studies done in Edo, Abia, Benue and Anambra States of Nigeria [9,
25,
28,
29]
with prevalence ranging from 9-13%. Contrary to this, other studies done in Ondo, Kano and different parts of Lagos, Nigeria [20,
30-33]
reported lower prevalence ranging from 2.8% to 7% though a Nigerian study by
Abiola et al [24]
have done in Lagos city observe a higher prevalence of overweight and obesity of 23.2%.
In the face of persistent under nutrition, obesity rates appear to be increasing globally, especially in many low- and middle-income countries that previously had a very low prevalence. [34]
This coexistence of underweight and overweight/obesity is being reported as the ‘double burden’ of malnutrition, which has been observed in countries undergoing nutritional transition especially developing countries were the dietary patterns are changing and becoming more western. [7,
35]
The level of awareness and knowledge of overweight and obesity among adolescence may be contributing to this increasing trend of over nutrition, where there is a lack of understanding of the risks factors and consequences of overweight and obesity and therefore the practice of inappropriate weight promoting behaviour. This may have contributed to the level of overweight and obesity prevalence observed in the present study, as a majority of the respondents (89.6%) had a poor to fair level of awareness and knowledge which appeared to follow a similar trend in a previous study that also reported a majority of their respondents (68%) having poor knowledge of the risk factors and problems associated with being overweight or obese. [9]
This poor level of knowledge may be attributed to the apparent collapse of school health programs that promote nutrition education in most schools in Nigeria. [36]
In the present study, age and gender were significantly associated with the nutritional status of adolescents which is consistent with a study done by Mustapha et al [20]
and also similar to a number of other previous studies to the extent that, they reported either age or gender as being significantly associated with nutritional status. [9,
25,
29,
33,
37-39]
But on the contrary, a number of studies reported a lack of significant association between age, gender and nutritional status of adolescents.[28,
30,
33,
40,
41]
Furthermore, adolescence is a period, when growth velocity increases and the body’s proportion changes substantially especially for women as they age, and this is affected by inadequate diet, unfavorable environment and living conditions which occur to varying degrees within and across regions and populations. [42,
43]
From the Nigerian studies reviewed, within the present study, it appeared that most of the studies with significant associations with either age or gender were conducted among adolescents from the Southern part of Nigeria while most, lacking any significant association were conducted among adolescents from the Northern part of Nigeria. This regional difference, if significant at all, may have contributed to the observed associations of age and gender with nutritional status in the present study and this observation should be further explored.
In the present study, the religious background of the adolescent and occupation of the adolescent caregiver were significantly associated with their nutritional status but this; observation was not consistent with studies done by Mogre et al [40]
and Mustapha et al [20]
who reported that there were no significant associations. Also in the present study, the household size in terms of number of siblings and the type of school attended by the adolescents were not significantly associated with nutritional status. Similarly, studies from Olumakaiye et al [19]
and Mustapha et al [20]
reported consistent findings with respect to household size but Abah et al [9]
reported a significant association with respect to type of school which was inconsistent with the present study. Even though, in the present study, the type of school was not significantly associated with the nutritional status, it was observed that there was a higher proportion of overweight and obese adolescents in private schools when compared to those in public schools which was also similar to the observations of Ebenezer et al. [44]
The factors assessed and found to be significantly associated with adolescent nutritional status in the present study, appear to be either structural or not easily modifiable such as age, gender, who the caregiver is, class level in school and birth position in the household. Therefore taking cognisance of these factors while identifying modifiable opportunities such as level of knowledge, which apparently was observed in the present study to be generally poor to fair amongst the majority (89.6%) of the adolescents, is a critical step towards effectively designing appropriate strategies with an integrated approach and multiple entry care points that will address adolescent malnutrition.
5.0 CONCLUSION
Many children, especially in developing countries, enter adolescence nutritionally disadvantaged and surrounded by unfavourable environmental conditions, socioeconomic status, lifestyle and eating habits that make them vulnerable to diseases; and if they survive death, they are plagued in adulthood with chronic diseases, disabilities, poor quality of life and subsequently, early death. So it is important to focus integrated nutritional strategies not only on children but also on adolescents. This will involve improving knowledge through effective communication and counselling that is accessible to the adolescents at multiple care points. Similarly, it will also involve promoting behaviour modification towards appropriate eating habits and lifestyle; and encouraging food diversification and fortification not only at the household level but in schools by establishing or strengthening existing school based nutrition programs.
Limitation of study
The use of chronological age instead of physiological age in this study, poses some challenges in the assessment of nutritional status in adolescents from developing countries when comparisons are made to the WHO reference population; and also, using the WHO growth charts as a reference for populations from developing countries like Nigeria instead of using local reference data which unfortunately is unavailable, presents further challenges, particularly in the overestimation of under nutrition.
We thank all the participants in this study and the research assistants; Agbaeze Grace, Onwuchekwa Ugochukwu, Babalola Babatunde, and Obiagwu Kenneth who helped during the data collection.
Authors’ Contributions: All the authors participated in the study.
Competing interest: The authors hereby declare that there are no competing interests.
Source of funding: There was no external source of funding.
REFERENCES
4.
Rees J M, Neumark-Sztainer D, Kohn M, Jacobson M. Improving the Nutritional Health of Adolescents-Position Statement - Society for Adolescent Medicine. Journal of Adolescent Health. 1999, 24:461-462.
12.
DeOnis M, Onyango A W, Borghi E, Siyam A, Nishidaa C et al. Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization 2007; 85:660-667.
15. Cochran WG. Sampling technique. 2nd ed. New York: John Wiley and sons Inc. 1963.
18. Leenstra T, Petersen L T, Kariuki S K, Oloo A J, Kager P A et al. Prevalence and severity of malnutrition and age at menarche; cross-sectional studies in adolescent schoolgirls in western Kenya. European Journal of Clinical Nutrition. 2005, 59: 41-48.