Original Research Article
Year: 2016 | Month: July-September | Volume: 1 | Issue: 3 | Pages: 1-7
Effect of Strength Training on Upper Extremity Function in Children with Hemiparesis
Sara Samir Mohamed Ali1, Faten Hassan Abdel Azim2, Mohammed Abdel Moneim El Sobky3
1Physiotherapist at Saudi German Hospital Cairo, Egypt .
2Professor of Disorders of Growth and Development in Paediatrics and Its Surgery, Faculty of Physical Therapy, Cairo University, Egypt.
3Professor of Orthopaedics, Paediatric Hospitals, Cairo University, Egypt. Fellow of the Institute of Orthopaedics, London University. Fellow of the British Orthopaedic Association,Member of European Paediatric Orthopaedic Society.
Corresponding Author: Sara Samir Mohamed Ali
ABSTRACT
Objectives: this study aimed to evaluate the effect of upper extremity progressive strengthening exercises on upper extremity function of hemiparetic children. Design: Randomized clinical trial. Subjects: Thirty children (17 boys and 13 girls) with hemiparetic cerebral palsy whose age ranged from four to six years participated in this study. They were classified randomly into two groups of equal number; control group (fifteen children: ten boys, five girls) who received a designed physical therapy program directed towards improving gait pattern and study group (fifteen children: seven boys, eight girls) who received the same designed physical therapy program given to the control group in addition to the designed progressive strengthening program for the affected upper limb.
Materials and Methods: Isometric strength of the affected upper extremity using Lafayette hand held dynamometer and QUEST (quality of upper extremity skills test) were measured from both control and study groups before and after ten weeks of treatment.
Statistics: Paired T test within the same group and unpaired T test between different groups were conducted to analyse collected data before and after 10 weeks of treatment. In order to identify differences between the two groups, a Mann-Whitney test was conducted on the changed amount to identify the difference between the two groups.
Results: A significant improvement was recorded in the measured variables in the study group when comparing their pre and post treatment mean values.
Conclusion: From the obtained results of this study, it could be concluded that progressive strengthening program is beneficial to improve upper extremity function in hemiparetic cerebral palsied children.
Key words: Strengthening exercises, Hand function, Cerebral palsy, Hemiparetic, Children.
INTRODUCTION
Hemiplegic cerebral palsy (CP) is one of the most common syndromes in full term children, and is the second in prevalence after diplegia in preterm infants (Feddrizi et al., 2003). Infantile hemiplegia is usually characterized by a good level of activity during childhood, and the affected child has a greater chance of having a less complicated adult life when comparing him with most types of CP (Scrutton 2000). In terms of activity and participation limitations there is a significant reduction of the effective use of the arm and hand in the activities of daily living due to the involvement of the upper limb more than the lower limb (Bax, 2005). The mechanisms of neuro-plastic re-organization of the sensory motor system can vary from those observed at later stages of development. This is typical when the lesion occurs at an early stage of development either during the intrauterine life or during early infancy (Eyre, 2007). In typically developing children manipulatory actions and performance of fine motor skills develop rapidly during the first years of life with a subsequent refinement occurring throughout childhood (Case-Smith, 1995). There are several contributing factors to hand skills development:
1)
Visual skills: the visuomotor development required for accurate reach matures by approximately 6 months of age. The infant visual motor coordination continues to refine, and by 9 month of age the infant guides the hand movement using somatosensory integration. (Bertenthal & Hofsten, 1998)
2)
Somatosensory function: the role of somatosensory information and feedback is critical to development of children’s hand skills especially those involving isolated fingers & thumb movement. By 2.5 years of age children can identify common objects by touch alone and by 5 years of age can demonstrate good haptic (knowledge of abjects gathered by mean of active touch) recognition of unfamilioar objects. By 6 years of age identification of three dimensional objects and perception of spatial orientation are well developed (Bunshnell & Boudreau, 1999).
3)
Sensory integration: sensory registration problems, tactile hypersensitivity, poor tactile discrimination and dyspraxia are the most likely sensory intergration problems affecting children with cerebral palsy combined with motor planning problems (Steenbergen et al., 2007).
4)
Visual perception and cognition: hand use and cognitive development seem to be particulary linked in infancy and early childhood. The child perception of object’s characteristics, movement speed required and power needed affects his or her ability to effectively control objects (DeLuca et al., 2003).
5)
Skeletal integrity: the integrity of the hand joint and bone structures is an important consideration in hand function. involvment of the thumb has a more significant effect on aqcuisition and use of hand skills than impairment in any other digit. Effective hand function also depends on efficient mobilization of distal muscle groups that control the palmar arches. Limitations in range of motion can occur as a result of muscle weakness, abnormal joint structures or other causes that affect the child ability to to grasp larger objects or to flatten the hand to stabilize materials (Smith & O’Brien, 2010).
6)
Muscle function: aspects of muscle functions are muscle power, muscle tone and muscle endurance. Sufficient strength is necessary to initiate all types of grasp patterns and to maintain these patternsduring lifting and carrying. Children’s grasp strength gradually increases through the preschool years, elementary school years and adolescence (Lee-Valkov et. al.,2003).
30 hemiparetic children participated where 15 were assigned to the study group and 15 to the control group. Sampling method was simple random sampling among the population of hemiparetic children aged from 4-6 years visiting the out clinic. Central allocation using the phone numbers was used for group allocation. Assessment and treatment sessions took place in the faculty of physical therapy at Cairo University and Al Shikh Zayed Al Nahyan general hospital from December 2014 to May 2015. Inclusion criteria were: Their chorological age ranged from four to six years, all children were able to walk independently without assistive device and the degree of spasticity ranged from 1 to +1 according to the Modified Ashworth Scale (Bohannon and Smith, 2004).
They were able to follow simple verbal commands or instructions included in both assessment and training procedures.
The child was excluded from the study if he / she had one or more of the following conditions:
1)
Visual or auditory defect that may affect their performance.
2)
Previous orthopaedic surgery for the affected upper extremity.
3)
Fixed deformities or involuntary movements (tremors, chorea, athetosis) that hinder the assessment and training procedures.
4)
Injection with botulinium toxin in the last 6 months.
Procedures:
Assessment procedures are done for both groups before and after 10 weeks of therapy and consist of Assessment of muscle strength using Lafayette hand held dynamometer and quality of upper extremity skills test (QUEST).
First the child is taught the direction of motion and the muscle action he is asked to do then, a trial is done with manual isometric resistance to assure that the child understands and is able to do the desired action. Readings for each muscle are taken 3 times in a row and their mean is calculated. Selected muscles were wrist flexors, wrist extensors, elbow flexors, elbow extensors, shoulder flexors, shoulder extensors, shoulder internal and external rotation.
QUEST is used to evaluate quality of upper extremity function in four domains: dissociated movement, grasp, protective extension and weight bearing. It was also done for each child pre and post 10 weeks for both groups. Tools needed were: quiet room, Chair or seating system, Table just above the waist level, Four one inch cubes, Cup, Regular size crayon or pencil, Blank paper, Cheerios cut into quarters, Mat, Small bench (optional), QUEST manual/ score sheet, Toys. The score must be entered in every scoring box even if the item is not tested (i.e., yes, no, not tested). Every effort should be done to complete the entire assessment. For any item the therapist is not sure of the child’s response or thinks the child is almost doing it, the score must be No.
Repetitive strengthening exercises: Study and control group have received the same selected physiotherapy program for the affected upper extremity which consists of: Neuro-developmental training (NDT), Hand-arm weight bearing and weight shifting and Stretching exercises. The study group received additionally, a designed program of resisted exercises for the affected upper extremity which consists of: Resisted fingers extension and abduction, Resisted wrist extension, Resisted elbow flexion and extension, Resisted shoulder flexion and extension, Resisted shoulder abduction, internal and external rotation. Exercise repetitions for each individual were set according to child repetition maximum for each muscle group. Maximum repetitions reached were 30 repetitions for each muscle group and session time ranging between 40-60 minutes according to child cooperation and numbers of repetitions the child can do.
Statistics:
Paired T test within the same group and unpaired T test between different groups were conducted to analyse collected data from both groups before and after 10 weeks of treatment. In order to identify differences between the two groups, a Mann-Whitney test was conducted on the changed amount to identify the difference between the two groups.
RESULTS
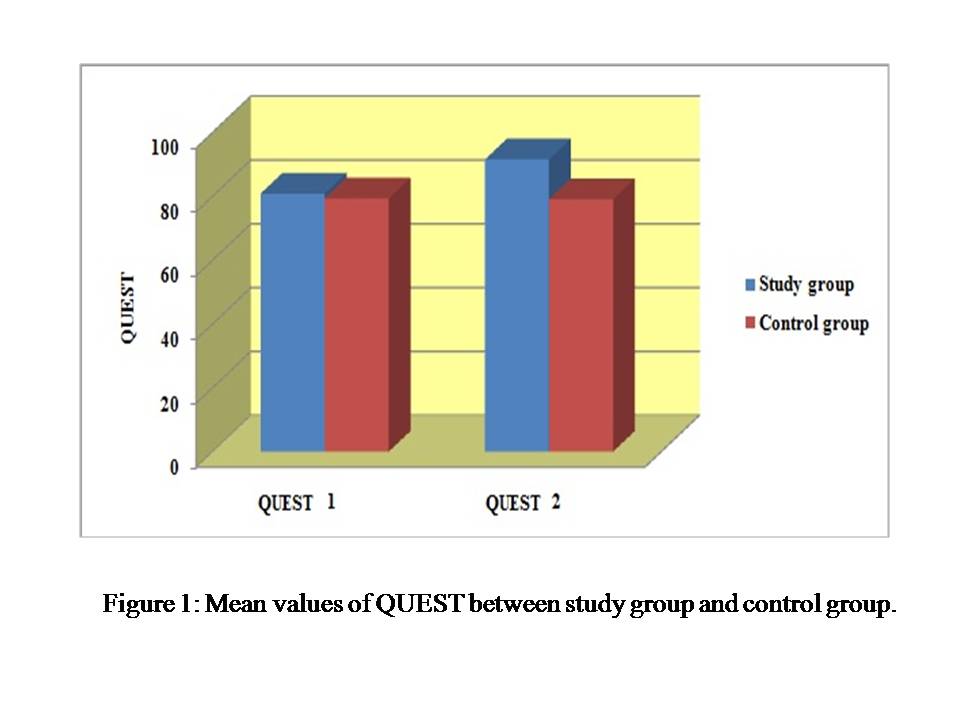
The analysis showed significant improvement in the isometric strength of the study group for the following muscles: wrist flexors, extensors, elbow flexors and extensors, shoulder flexors, extensors, abductors, internal and external rotators (Table 1). QUEST also showed significant improvement in all four categories of upper extremity function using Wilcoxon signed ranks-test (Table2). (Figure 1) shows mean values of QUEST between study group and control group which underlines the improvement in upper extremity function after 10 weeks of repetitive strength training.
Table 1 Difference in mean, standard deviation and level of significance of isometric muscles strength before and after treatment in study group.
|
Iso. Ms Strength pre |
Iso. Ms. Strength post. |
Significance level |
W.F. |
0.82 ±0.27lb |
4.20 ±0.27lb |
P = 0.0001; P<0.05 |
W.E. |
0.76 ±0.15lb |
0.76 ±0.15lb |
P = 0.0001; P<0.05 |
E.F. |
1.20 ±0.46lb |
4.65 ±0.29lb |
P = 0.0001; P<0.05 |
E.E. |
1.31 ±0.71lb |
4.52 ±0.23lb |
P = 0.0001; P<0.05 |
Sh.F. |
1.33 ±0.55lb |
4.41 ±0.24lb |
P = 0.0001; P<0.05 |
Sh.E. |
1.21 ±0.48lb |
4.44 ±0.32lb |
P = 0.0001; P<0.05 |
Sh. Abd. |
0.96 ±0.34lb |
4.21 ±0.25lb |
P = 0.0001; P<0.05 |
Sh. INR. |
1.03 ±0.33lb |
4.15 ±0.27lb |
P = 0.0001; P<0.05 |
Sh. EXR. |
0.86 ±0.23lb |
4.24 ±0.26lb |
P = 0.0001; P<0.05 |
Table 2. Difference in mean, standard deviation, P and Z value of QUEST in the study group.
|
QUEST |
|
QUEST 1 |
QUEST 2 |
|
Mean ± Standard deviation |
80.85 ±5.68 |
91.54 ±3.07 |
Minimum to Maximum |
70.63 – 88.76 |
86.82 – 96.12 |
Z-value |
3.059 |
|
Level of significance (P-value) |
0.002 |
|
Significance (P<0.05) |
S |
|
Figure 1: Mean values of QUEST between study group and control group.
{kind=link}
DISCUSSIONS
The present study was conducted to study the influence of strength training on upper extremity function specially the hand function in children with hemiparesis.
The age of children participated in this study was selected from 4 up to 6 years old to be able to follow instructions during assessment and treatment procedures. In this study the children with hemiparesis received strength training for the upper extremity for 10 weeks long, day after day for 40- 60 minutes per sessions. Results showed significant improvement in muscle power and upper extremity function and grasp.
These results agree with (Rameckers et al., 2015) (Eun-Young et al 2014) and (SCHOLTES et al., 2008) Eun-Young Park et al. (2014), investigated the evidence that strength training can improve muscle strength and functional abilities in individuals with cerebral palsy. The search focused on studies that applied strength training for children with cerebral palsy for which six electronic databases were used to extract literature published from 2001 to 2012. The study concluded that strength training is useful for improving muscle strength in individuals with cerebral palsy, specifically in youth and children, and optimal exercise consisted of 40- to 50-min sessions performed 3 times per week. The author also recommended that more studies that are rigorous are needed to determine the contributions to gross motor function despite the results that prove the strengthening interventions to be effective in improving activities, including gait.
A recent systematic review (Franki et al., 2012), however, concluded that muscle strengthening improved the level of body structure and function (i.e., strength), and activity without adverse effects in children with CP. Franki also reported that the evidence for the effect of strengthening is insufficient. Recently, strengthening is adopted widely by clinicians to improve muscle strength and motor function in children with CP (Lee et al., 2013; Scholtes et al., 2010).
Mockford and Caulton (2007) conducted a systematic review to test and find the evidence concerning the effects of progressive strength training on function and gait in ambulatory children and adolescents with CP and concluded that function and gait improvements were greater in pre-adolescents. Scianni et al.’s (2009) meta-analysis of five studies concluded that strengthening interventions are not effective with cerebral palsy children.
Rameckers et al. (2015) conducted a systemic review to investigate the effects of strength training of the upper limb in children with Cerebral Palsy (CP). The studies strengthening intervention were divided in two categories: those based on strength training only, and those on strength training combined with other interventions. From these studies the author concluded that there is no clear method of training can be advised. Both stand-alone or strength training in addition to other modalities showed equal effects. Combining task oriented therapy and electrical stimulation did not reduce the effect of training. According to results of this review a minimum frequency of 3 times per week was performed in all studies and duration of 8 weeks a least seemed to be effective for strength training. Rameckers also recommended performing RCTs in the field of strength training of the upper limb in children with CP, using specific guidelines for strength training as a start to standardize the training principles. From a clinical point of view it is very important to know if the increase in strength due to training is associated with meaningful change in children’s independence / abilities. Faigenbaum et al., 2009 recommended training at least 12 weeks long, 3 times per week, with 8-15 repetition maximum as resistance. The Author also highlighted the need to study the outcome of strength training on function and participation areas, in relation to activity goals the children want to achieve.
Dong-A Kim et al., 2012 studied the effect of comprehensive hand repetitive intensive strength training (CHRIST) on upper limb function in children with cerebral palsy using motion analysis. The subjects in this study included 19 children (10 males, 9 females, mean age=8.8 years) with cerebral palsy. The experimental group (n=10) received CHRIST and general rehabilitation therapy. The control group (n=9) received a home program as well as general rehabilitation therapy. Both groups received 30 sessions of CHRIST or home program training for 60 minutes per session 3 times a week during the 10-week period. The reaching movements were captured by a motion analysis system. Kinematic variables including movement time (MT), mean velocity (MV), normalized jerk score (NJS), mean angular velocity (MAV) and normalized jerk score of the shoulder, elbow and wrist joint with comfortable and fast speed were analyzed between groups and the pre-post training group. After pre- and post-training experimental group, MT, MV, NJS, MAV of shoulder, elbow, wrist and NJS of elbow and wrist improved significantly in reaching movement of both comfortable and fast speed (p<0.05). However, After pre- and post-training control group, MV improved significantly in reaching movement of only comfortable speed (p<0.05). Between two groups, MT and MAV of the elbow at comfortable speed and NJS of the elbow at fast speed were statistically significant (p<0.05). CHRIST proved to be an effective intervention for improving upper limb extremity function of reaching movement in children with cerebral palsy.
CONCLUSION
In this study, a total of 30 children with cerebral palsy were selected. 15 children in the experimental group received upper extremity repetitive intensive strength training and general rehabilitation 30 times in ten weeks. However, 15 children in the control group were given general rehabilitation. The upper extremity function and the isometric muscle strength between before and after treatment of each group were compared. The group that received upper extremity repetitive intensive strength training showed a significant difference for the upper extremity function using QUEST since there was a significant improvement of the upper extremity muscles strength. This objectively confirms that upper extremity repetitive intensive strength training is a treatment that is helpful to enhance upper limb strength and function. Utilizing upper extremity repetitive intensive strength training is highly suggested as a rehabilitation treatment that enhances capability of exercising for upper limbs of children with cerebral palsy with special focus on functional improvement. Further more specific randomized control trials are recommended to study the effect of strength training on upper extremity function in different types and ages of children with cerebral palsy with a special focus on participation in school and sports activities.
REFERENCES
·
Hoffman, J.R., J. Kang, N.A. Ratamess, M.W. Hoffman, C.P. Tranchina, and A.D. Faigenbaum. Examination of a high energy, pre-exercise supplement on exercise performance. Journal of international society of sports nutrition 2009; 6:2.
·
Jodi Crompton; Mary P Galea; Bev Phillips. Hand-held dynamometry for muscle strength measurement in children with cerebral palsy. Developmental Medicine & Child Neurology 2007; 49: 106-111.
How to cite this article: Mohamed Ali SS, Faten Hassan Abdel Azim FH, Moneim El Sobky MA. Effect of strength training on upper extremity function in children with hemiparesis. International Journal of Science & Healthcare Research. 2016; 1(3): 1-7.
**************